
Misc. Mental Musings
Weighing Weight Loss
S. G. Lacey
Wacky Wording:
Danuglipron. Mounjaro. Ozempic. Wegovy. Zepbound.
Is this the itinerary for an African safari? Or the next wave of modern medicine?
Unfortunately, the latter. However, drinking the fermented sugar cane beer of Gabon, hiking to the top of Mt. Kilimanjaro, lazing on the sandy beach along Mozambique’s east coast, adopting a diet of cassava and curry in Nairobi, or going on safari across Zambia, may be healthier alternatives.
The purveyors of these products, while not exactly household names, are at least easier to pronounce than the myriad drugs they manufacture and market.
Eli Lilly. Novo Nordisk. Pfizer. Apparently, high level marketing executives use the same tricks of rhyming, alliteration, and malapropism in their corporate monikers as they do for proliferating pills.
Granted, the COVID-19 pandemic, and subsequent vaccine development, have made a few of these biopharma conglomerates more common in the public lexicon.
The goal of these goofy designations is to elicit interest, explain functionality, and enable approval. With over 30k proprietary medicines in the United States alone, unique letter combinations and novel sounds are hard to come by. Etymology. Linguistics. Meaning. Onomatopoeia. Symbolism. Whimsy. All literary elements are in play during the drug naming process.
The word salad listed above represents the most popular in a growing list of weight loss medications. These treatments are being taken with increasing regularity by an increasing swath of the American population. Understandable, considering the unfavorable health statistics across the United States.
Is this new medical technology for rapid weight loss a boon or a bust? As the famous Jurassic Park movie quote goes, sometimes it’s not question “if you could do something, but if you should”. Especially with regards to ingesting foreign substances into one’s body. As it turns out, there’s a lot of nuances to this debate, with many of the key facts still coming to light.
Way Back When:
Many paranoid people in the populus are concerned about invasive pharmaceutical intervention in their everyday lives. However, scientific discoveries that substantially improve health and wellness isn’t just a recent phenomenon. Throughout history, medicinal treatments have been a staple of human civilization advancing and developing.
Before getting worked up about this modern wave of weight loss drugs, it’s valuable to look at how enterprising persons have pedaled their wares to the masses in the past.
Over time, medical practitioners have taken various names: druids, sages, alchemists, shamans, medics, healers, doctors. With shifts in time and place, not only have the monikers of these individuals changed, but so have the tools and treatments available to them.
Initial homeopathic remedies were made with natural herbs, available locally, and blended arbitrarily. The next evolution was identifying key active ingredients, grinding these elements into fine powders, then mixing in carefully measured ratios.
As the globe industrialized through machinery, pills, like nearly every other consumer product, became mass produced, and thus more consistent. In this modern era, computing power has ushered in a wave of advanced diagnostic analysis and chemical modeling.
The pace of change in the medical profession is ramping up rapidly. Scientists and doctors are entering new fields, and examining new solutions to all manner of diseases and disorders. Including one of society’s most prevalent ailments. Obesity.
As it turns out, American culture has a long history of fascination with weight loss drugs.
The world’s first experience with medicating their mass was not surprisingly cryptic and complexly named. This seems to be a trend within the weight management industry. This initial product, with the chemical classification 2,4-dinitrophenol, was discovered during World War I. Originally developed as an explosive component for creating munitions, factory workers handling it were observed to lose substantial girth.
At the beginning of the 1930’s, DNP was rebranded as an anti-obesity therapy. Within years, more targeted health research on patients showed high doses could cause blindness, neurological issues, and even death. By 1938, the treatment came under increased scrutiny, and was banned by the U.S. Food and Drug Administration. Another common legislative theme which plays out time after time in this specific scientific space.
Another war, another weight management solution. Benzedrine, more commonly known as amphetamine, after proliferation during World War II. Benzedrine salts were a powerful stimulant used by soldiers on all sides to stay awake during grueling combat routines. Apparently, times of tumult lead to medical developments.
After the conflict, pharmaceutical company Smith, Kline, & French, now biotech behemoth GlaxoSmithKline, commercialized these prescriptions for common citizens. Marketing materials specifically targeted the burgeoning housewife demographic, as part of the 1950’s household formation and baby boom, using a marginally factual newspaper campaign. The basic concept of increasing metabolism, facilitating more bodily movement, and thus burning fat, has been tried in all sorts of diet drugs since then. [REF]

The amphetamine mixed salts approach expanded in future decades. It just needed some savvy rebranding to really take off. Which came in the form of colorful rainbow diet pills, an aesthetic that perfectly matched the 1960’s decade.
In 1960, Obetrol, a combination of methamphetamine and dextroamphetamine, was approved by the FDA as an obesity medication. The harmful impacts, especially with the “meth” component, were quickly discovered as usage expanded, but didn’t end biomedical innovation in this space.
Numerous form factors were created: pills, drops, inhalers, and injection. By 1970, just a decade later, 5% of all Americans were on an amphetamine prescription. Some of this usage was related to the recreation drug element of Obetrol, with hallucinogenic experiences common based on the dosage amount and mode of intake. It also helped from a sales standpoint that the product was highly addictive.
Obetrol was reformulated several times, eventually rebranded as Adderall, the well-known ADHD treatment, with no associated fat burning claims.
A similar clever marketing ploy continued in the next batch of miracle anti-obesity drugs, dubbed fen-phen, which was released in 1985. This class of drugs combined fenfluramine and phentermine, hence to the catchy product name.
Both these active ingredients were shown to provide weight loss on their own. What could possibly go wrong with a combination cocktail? At least this offering came with more explicit dosage protocols. Since people are so good at following doctor’s orders on their own.
This potent treatment wasn’t supposed to be used for more than straight 12 weeks. After this duration, especially in women, elevated serotonin levels started to cause heart valve issues. An untreatable, deadly, heart failure is an unfortunate side effect for a lady with a slightly overweight condition.
Fen-phen was pulled from the market, resulting in a multi-billion-dollar legal settlement by parent company Wyeth in 1999. This is one of the few times where big pharma companies have been forced to pay for medical malpractice transgressions that they knew about, but kept hidden.
Time for a quick run through on weight loss products and side effects of the 21st century offerings.
2000 brought Xenical, an orlistat, which promoted fat digestion, with 30% of this unwanted gelatinous material passed through one’s stool as an oil. Issues with basic bowel control understandably hindered product proliferation.
Belviq, a lorcaserin, was launched in 2012. This concept sought to suppress appetite, specifically by engaging the serotonin receptor in the hypothalamus. This novel approach was one of the first to leverage mind manipulation as opposed to physical means, but was unfortunately pulled after just 8 years, due to cancer concerns. Often, it takes decades of clinical trials and patient usage for important and undesirable side effect to arise. Thus, for Belviq, it’s stint in the market was impressively short.
Many folks are aware of these various pill products foisted on the portly populus in recent decades. The absurd drug names, and troubled success rate, are a testament to the failures of the biotechnology industry to achieve their fundamental goal. Helping humans get healthy.
Lastly, and most relevant to recent drug developments, in 2005, exenatide and liraglutide formulations were invented, becoming the precursor for contemporary GLP-1-RA diabetes treatments. These offerings were administered in lower doses, and thus required more injections, and inconvenience, for patients.
Still, these early formulations were a proof of concept for this novel technology breakthrough. The semaglutide approach, with higher dosage, now yields noticeable weight loss benefits for a diverse group of individuals. How is this impressive feat possible?
Witty Wisdom:
Time for a nerdy chemistry discussion. In an effort to understand what makes semaglutides so powerful for weight loss. It turns out scientists are still trying to figure out these minor details.
While GLP-1-RA is now being generated synthetically in modern biotechnology labs, it also occurs naturally in the wild. Fortuitously, Gila monster venom contains this unique chemical composition, which allows regulation of digestion, and a sensation of fullness. This technique enables these lazy lizards to survive in their harsh desert environment, only needing to ingest a half dozen or so meals a year, relying on a slow metabolism, while living off the fat stored in their tails. [REF]

This same mechanism has proven valuable for regulating insulin and glucose levels in humans. In 2005, the FDA approved the drug Byetta, for management of type 2 diabetes. The active ingredient, protein exendin-4, was isolated from the Gila monster’s venom. For diabetics, this treatment works by lowering blood sugar and subduing appetite, replicating the functionality of the naturally occurring GLP-1 hormone.
As luck would have it, there’s a convenient side effect of the hunger suppression and slower digestion offered up by semaglutide-based treatments. Weight loss.
Scientifically speaking, a semaglutide is a glucagon-like peptide-1 receptor agonist. Now it makes sense why the GLP-1-RA acronym has come to vogue, from a pure simplicity of communication standpoint. Essentially, synthetic semaglutides replicate the function of organic peptides, binding to the receptor, and stimulating insulin discharge through the incretin effect.
Typically, when a human consumes food, various polypeptides are secreted from the intestines into the bloodstream, then attach to beta cells which produce insulin in the pancreas. For patients with type 2 diabetes, this process can be blunted, or even absent. Through supplemental GLP-1 injection, impaired individuals can revive their ability to excrete insulin, an important regulatory tool for the body.
Importantly, GLP-1 receptors are found on the lateral hypothalamus, a region of the brain associated with many key functions, including water intake, feeding control, and sodium excretion. All these elements are obviously associated with weight management.
Even more interesting, this same lateral hypothalamus region is directly responsible for mental reward tracking and success stimulation in humans. Finally, the pharmaceutical industry has found a treatment that influences the emotional element of eating, specifically with regards to impulsive intake.
Retatrutide, a triple peptide, which represents an even more complicated chemistry, could be the next level of advancement in this burgeoning field. Who knows what biotechnology innovation firms, buoyed by funding from big pharma, will come up with in the future. It’s clear that demand, and desire, is high in today’s society.
Why It Works:
Science is complicated. Which is why we’re still learning about an affliction as prevalent and invasive as obesity. In fact, being overweight wasn’t even acknowledged as an issue until the turn of the recent millennium.
The National Institutes of Health, or NIH, was the first medical organization to categorize obesity as a disease, in 1998. It’s governmental body acronym counterpart AMA, better known as the American Medical Association, debated this claim for over a decade, citing lack of symptoms and true bodily harm, before finally conceding in 2013. This opened the door for all manner of new pharmaceutical treatments in the weight management space.
The previously mentioned orlistat family of drugs, developed in the early aughts, were the first mainstream offerings to take advantage of this aligned legislative stance. The strategy for this treatment was simply reducing the body’s ability to absorb fat. While this brute force mechanism was not very successful, its retail introduction led scientists to explore new mechanisms for controlling weight.
Another common supplemental weight loss treatment is thyroid hormone treatment. While this technique can be more effective than just diet or exercise, it turns out fat isn’t the only thing patients lose. Clinical trials with thyroid hormone have shown over time users exhibit loss of muscle and bone as well. Plus, increased risk of heart problems. Not exactly great marketing material.
There’s another, much more proactive, approach for shedding the pounds. Surgical operations like bariatric surgery, gastric bypass, or tummy tucks. These invasive procedures are much less desirable, and don’t scale very well, due to lack of skilled doctors in this field. Less than 1% of eligible patients elect for such a metabolism management operation, and, until recently, just 2% of obese individuals have opted for any of the many weight loss medications available to the general public.
Per medical research, there’s a known prioritization of beneficial weight loss activities: diet, then exercise, then drugs, then surgery. It’s also important for these habit changes to be persistent and permanent, if a lifelong bodily effect will materialize and be maintained.
Some newer alternative mass management strategies include caloric restriction through fasting, minimally invasive endoscopic procedures, and electrical stimulation via an implant. While better than going under the knife and requiring months of painful recovery, none of these options are overly compelling. Thus, a simpler weight loss solution is needed to entice the masses.
Enter GLP-1-RA treatments, which are easy to administer, and encourage fat loss through a multi-pronged approach.
First is the traditional mode of increased metabolism, a tried-and-true technique for burning fat. This is akin to the numerous amphetamine salt drugs of the past, supplements which are still popular within the bodybuilder ranks.
The next system is a physical mechanism, which slows emptying of the stomach. While promoting gas build-up, this is a more pleasant approach than the steady leaking caused by the orlistat category of drugs. As they say in the TV commercials, side effects may vary.
The most important breakthrough provided by GLP-1-RA chemistries, supplementing these known digestion mechanics, is a secondary strategy. Mental appetite fulfillment, which is more of a wholistic body and mind condition. Satiety, a medical term slightly different in meaning to the more common satiation, implies a sense of fullness between meals, rather than while ingesting. It turns out humans, and most other mammals, don’t eat if they don’t feel hungry. Apologies to our overzealous canine friends.
The GLP-1 hormone acts on many elements of the hypothalamus. This zone affects the brain’s ability to monitor circadian rhythms, and also has an influence on dopamine, the body’s pleasure center. Imagine being able to feel like you just finished at entire juicy burger and side of salty fries for dinner, after just a few small bites at lunch. And, the morsels may taste nothing like the glorious and greasy fast food remembered from your youth. OK, maybe we have quite reached the desired utopian future yet.
The reason why these drugs influence the actual taste of food is still being explored. But it’s hard to argue with the clinical results regarding improved health. The performance of new semaglutide treatments in large scale trials is truly staggering.
In a seminal 2022 study, patients exhibited 15% weight loss over the course of just 68 weeks. While the rate of reduction eventually leveled off, during the entire 2-year duration, patients averaged a 15.2% drop in body mass for the semaglutide treatment, versus only 2.6% for placebo control group. This test doesn’t demonstrate long-term efficacy, but is a provable result, with findings well outside of error bars, as shown in the graph below. [REF]

Granted, these trials were funded by Novo Nordisk, using their own Wegovy product. A follow-up, independent, clinical study had similar findings, though shorter in duration. Over 30 weeks, participants cut 5% of their body weight, and 1.6 inches off their waist. An impressive, unbiased, confirmation of medical success.
During these various research endeavors, 80% of tested patients complained about adverse gastrointestinal issues: constipation, diarrhea, nausea, and vomiting. In contrast, just half of the control group reporting these same symptoms.
While unpleasant, these uncomfortable experiences are a far cry from fatal ailments, and didn’t reduce the study pool significantly over the lengthy research period. Considering the drastic observed weight loss results, obese individuals seem more than happy to endure a few digestion discomforts. The opportunities for wholistic bodily improvement are vast, and compelling for many.
Where’s The Weight:
Never in the history of homo sapiens’ existence has the overweight problem been so acute. Or even an issue to consider. For several millennia, people were simply trying to get enough sustenance to avoid starvation; executing a difficult lifestyle in which energy expenditure often outstripped consumption.
Therefore, obesity is a product of the modern age, the first time when some developed segments of civilization have uninhibited access to food. Also, current daily activities don’t provide nearly enough natural exercise. We’re now trying to solve for a problem of our own making.
While body mass management has become a global issue recently, due to this combination of prevalent sustenance and sedentary lifestyles, there’s one country where obesity is truly an epidemic. Which happens to the most affluent nation in the world. The United States.
It’s estimated that 38% of the worldwide population is overweight or obese. Unfortunately, this metric of mass is nearly double within the U.S. cohort. Clearly, a safe and speedy solution is needed.
74% of Americans are now classified as overweight, obese, or extreme obesity, per Centers for Disease Control and Prevention research, with 42% falling in the latter two, more worrisome, categories. These body metrics are quite stringent, but based on historical health data for the entire human population.
For reference, the average American male is 5’-9” tall, and weighs 199.8 pounds, while the mean female is 5’-3.5” in height, and 170.8 pounds in mass. Per CDC guidelines, the upper weight threshold to avoid being classified as overweight at these standard heights is 162 and 138 pounds, for men and women, respectively. Thus, there’s a lot to lose.
Another huge issue in the United States is the inequitable distribution of obesity on several key metrics. Age, gender, ethnicity, income. Many of these factors are linked in our society, and follow well-known geographic breakdowns, as portrayed in the following state by state map. [REF]

Obese individuals are 80 times more likely to develop type 2 diabetes than health adults. This is why the rapid weight loss element is so critical for GLP-1-RA treatments.
As with any lifestyle improvement approach, it’s important to combine semaglutide usage with supplemental diet and exercise, per the pharmacy mandated protocols. Another important distinction is differentiation between weight and health. Some individuals who measure as overweight still don’t develop long-term adverse consequences. They’re just big boned, as the saying goes.
Realizing the healthcare crisis, and massive market opportunity, advertising for new weight loss drugs like Ozempic is widespread, employing all manner of clever tactics. This Novo Nordisk product’s catchy name can be found in every broadcasting format: magazines, billboards, commercials, social media, even traditional radio blurbs. The audio format, with predictable earworm jingle, is especially annoying.
This drug is now a social media sensation, with all sorts of skewed messaging on Tik-Tok, YouTube, and Instagram. Currently, there are 4X more Facebook and Instagram ads for Ozempic than Viagra. And the drug is mentioned by name in over a billion TikTok impressions; granted many of these shorts are amusing memetic statements, as opposed to actual semaglutide endorsements.
It’s clear the GLP-1-RA category of remedies is already a cult phenomenon, incredibly popular amongst the rich and famous. Who are currently to only folks that can afford the high price tag.
This product success is a testament to the incredible marketing departments at large biotech companies. They realize the immense profits which can be garnered if their drug is first to the shelves, and becomes a market leader within the diabetes and obesity categories.
The big pharma lead dog in this space currently is the aforementioned Novo Nordisk, who’s has executed a massive marketing campaign, through their army of sales reps, over the past few years. In 2022 alone, this company spent $9 million purchasing meals for over 450k doctors who prescribed their Ozempic and Wegovy products.
This corporate rewards campaign is supposedly tied to technical educational efforts regarding GLP-1-RA treatment benefits. Educating medical professionals on how to get fiscal kick-backs, clearly.
In an odd twist of fate, due to pervasive public advertising, patients are requesting specific semaglutide products by name from their doctors. This is a stark contrast to the upstream practitioner sales schemes proliferated by pharmaceutical companies in the past. They can now go with a direct-to-consumer model. A new way for huge drug conglomerates to take advantage of innocent consumers, leveraging the ills of social media.
There’s a risk that off-label semaglutide usage explicitly for weight loss means could lead to shortages, endangering the diabetic patients who actually require the treatment to function on a daily basis. Side effects for healthy folks are unknown, since this cohort wasn’t part of the curated clinic trials. Any unknown risks will be discovered over time, likely playing out under the bright and harsh public lens.
Wishful Wanderlust:
Life is not easy. Sometimes short-term suffering is an essential part of long-term success. This argument has been made by many haters of these new weight loss drugs. It helps to look back at the history of civilization’s advancement before trying to draw a line in the sand with regards to health and wellness.
Our ancestors used to die of the Black Plague, during the cold and dark medieval era, and the Spanish Flu, an ailment which had nothing to do with the country of Spain, and polio, solved by the novel vaccine work of Dr. Salk, and pneumonia, which still rears its ugly head seasonally. Our modern, domesticated life could be a lot worse.
We still lose several millions of humans globally each year to heart disease, stroke, respiratory infections, and cancer. Risk associated with nearly all these chronic conditions increases when individuals are obese. Thus, there’s plenty of logical motivation for the most self-absorbed country in the world to lose weight.
The prospect of getting slimmer and svelte, especially without any diet or exercise sacrifices, has captivated America society for decades. As discussed previously, most of these pipe dreams didn’t materialize. It turns out magic pills aren’t exactly magic. But now, a new contender has entered the fray.
The GLP-1-RA based weight loss medications have proven to offer help beyond simple biology benefits. The direct hypothalamus engagement means there’s potential these treatments can be used to fix many types of human addiction, through psychological manipulation means.
In clinical trials, patients imbibe in less booze, cigarettes, and snacks, opting for healthier foods and more exercise. No wonder scientists are calling semaglutides a wonder drug. Long term, it’s possible this class of medications could be formulated to combat other common compulsions. That’s the valuable benefit of a chemistry which acts on the mental mechanism that controls individual will power.
The incredible 15% - 20% weight removal capabilities of these GLP-1-RA systems can allow for substantial quality of life benefits. Not having to constantly think about mass management provides patients with the brain bandwidth to focus on other elements of their life, which epitomize the American experience, especially around the holidays: socializing and sex, shopping and sleeping.
The past few years has seen an explosion in new prescriptions amongst patients with no prior history of diabetes. These individuals skew younger, with 2/5ths between 25 and 44 years old, and towards women, as 4/5ths are female. This cohort is definitely not the group typically associated with adult-onset diabetes, but instead are just entering the mature phase of their life.
The struggle with physical image is especially acute for women; carefully curated images portrayed by actresses in the entertainment industry are impossible to replicate. The pressure to conform to aesthetic norms has changed over the years with shifting gender roles, but still remains a substantial societal factor.
Recent inclusive physique trends like “slim thick”, “body positivity”, and the “Brazilian butt lift”, have all proven to be fleeting, with the siren’s song of a rail thin, yet well-endowed, model ever-present. Perpetual social media post bombardment amplifies this persona of success and sexiness.
Now, there’s an easy way to achieve the desired feminine form. With just a simple shot.
Ozempic, and its various copy-cat treatments, offer up a very manageable means of application. A single dose, taken weekly, makes these drugs a godsend, especially when compared to standard, high-maintenance, insulin monitoring devices for type 2 diabetes. While the Ozempic strength ramps up over time, minimal side effects are experienced by most. And for many users, new to the diabetes diagnosis, they’ve never known anything different.
In the past, the injection form factor has been a deterrent, especially for squeamish patients. Now, folks are overcoming this fear, treating the needle applicator as a badge of courage. As they say, the ends justify the means.
The shift in psychology around food is a key part of how these semaglutide drugs work. Individuals who used to eat 3 full meals, with numerous snacks interspersed, are now content with just a light breakfast, and a simple dinner. This revelation makes finding and managing food intake no longer a chore. Perfect for the aspiring young performer, who’s always on the move between auditions and film sets.
The breakthrough moment for the GLP-1 movement came when it entered the Hollywood gossip scene. The epitome of this trend was when Jimmy Kimmel commented on the good looks of the crowd at the 2023 Oscars, a monologue during which he specifically referenced Ozempic.
These days, there’s lots of rumors, theories, and conjecture flying around in the tabloids. How did Kim Kardashian fit into that Marilyn Monroe dress? What doctor is handing out unquestioned semaglutide prescriptions around Los Angeles? Isn’t Elon Musk looking lean since he started taking Wegovy? [REF]
Entertainment is a field where success is directly tied to looks, so the high price of prescriptions can be easily justified. Especially for the uber-rich. Commoners can fend for themselves.

What’s The Cost:
The only thing more valuable than custom clutches and bougie booze these days are popular pills. In each case, indulgence is the name of the game. In fact, a yearly prescription of Ozempic retails for more than a fine watch or jewelry piece.
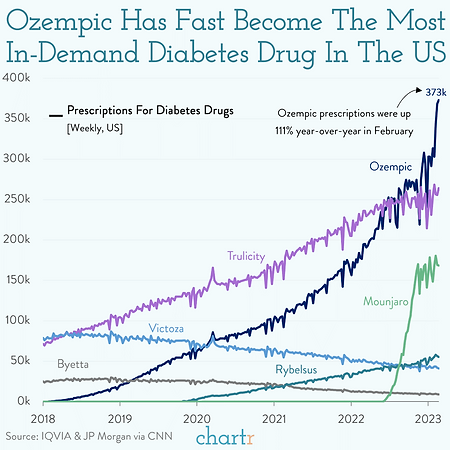
Demand for the leading diabetes treatment options, Ozempic from Novo Nordisk, and Mounjaro from Eli Lilly, is skyrocketing, as shown in the graph below. Apparently, the number of type 2 diabetics in the United States is increasing rapidly. Or maybe, there’s another, alternatively motivated, category of new users. [REF]
All these GLP-1-RA products are currently very expensive, with rules for insurance coverage still being hashed out. The incredible demand from consumers, and relative lack of supply until more FDA approvals arrive, continues to fuel this excessive pricing.
The absurd cost of semaglutide medications is what makes the large number of individuals already on this treatment plan even more impressive. The retail tab for Novo Nordisk’s Wegovy is $1400 per month to get the standard weekly dose allotment. Fortunately, for those covered by insurance plans, 80% of people are paying just $25 per month. However, getting the requisite doctor’s note, and being part of a medical plan that covers obesity treatment, is difficult.
Welcome competition is entering the space, driving costs down. Zepbound incorporates the same tirzepatide chemistry as Mounjaro, but is approved by the FDA specifically for weight loss treatment. This offering is a relatively cheaper $500 per month, provided one uses a savings card conveniently provided by the injection’s producer, Eli Lilly.
Plus, there’s now lots of knock-off GLP-1-RA products, manufactured and distributed through a multitude of shady means. These can be bought on the dark web anonymously, and without a prescription. A monthly fake allotment is roughly $600, while real Ozempic costs $900 per month without any insurance support. These are big numbers, equivalent to a car, or even apartment, payment.
The under-the-table offerings are often generic semaglutide formulations, which require users to mix their own solution, then inject via any available means. Not exactly boiling heroine on a spoon, but there’s definitely risk of misuse, and mistakes. In contrast, Ozempic is packaged in a simple, slick, sky-blue, delivery device.
Lastly, many individuals who aren’t explicitly overweight are using these treatments to improve their image; physical beauty is engrained in our culture. This is not a magic pill for wellness, but can provide a start to achieving a healthy lifestyle. The question is, how should these drugs be fairly and effectively distributed, until there’s enough pharmaceutical product for everyone who wants some?
There’s a conundrum between the acceptance-of-self movements, which have come into vogue over the past decade, and the recent seeming ease of losing weight with new GLP-1-RA treatment options. The concept of comparative vanity is decidedly a human trait, which can never be completely eradicated.
This category of drugs has been used sparsely as an off-label obesity treatment for years. The recent rapid increase in popularity has resulted in short supply for diabetic patients in need. Soon, doctors, insurance companies, and drugmakers will need to make tough decisions about equitable access to GLP-1-RA medications, both for the original diabetic cohort, and those newcomers seeking the ancillary weight loss benefits. Either way, there’s plenty of money to be made.
Wily Corporate Ways:
This is not the first time that seemingly beneficial drug treatments have been touted through clever marketing. Often throughout history, these medical cons turn out disastrous for many users over the long term.
Obetrol, the exogenous obesity treatment which gained popularity in 1960’s America, was one of the first big pharma coups of the modern era. Doctors could buy tablets in bulk for $70 per container, then break the package down, and sell the individual pills to prescribed customers for a $12k total haul. A pretty solid financial motivation to bend the rules.
If this scam sounds familiar, it is. Essentially the exact same ploy, with more aggressive marketing, and even higher peddler profit margins, was executed by Purdue Pharma while proliferating their OxyContin tablets 4 decades later. The transgressions of major drug companies and perpetual, and predictable.
There’s one element of American capitalism system that can provide insights into the future. Most of the time. The stock market. Since the recent explosion of these novel weight loss drugs, Mr. Market is sending some very clear signals. By crushing any food maker even remotely tied to selling snacks, sweets, or spurges.
Meanwhile, the valuations for drugmakers playing in the obesity realm have gone parabolic. Just look at Novo Nordisk, a Danish pharmaceutical company, maker of both Ozempic and Wegovy. This lone semaglutide technology has boosted them into the top echelon of European equities.
This operation, trading under the ticker NVO, recently became the largest market capitalization company in Europe, surpassing LVMH, whose suggestive symbol includes famous brands Louis Vuitton, Moet, and Hennessey, among other luxury offerings. Current stock valuations are often based on projected future sales, as opposed to actual revenue now. Novo and other players in the GLP-1-RA diabetes treatment and tangential obesity realms are certainly poised for growth. By shrinking patients.
Since Ozempic launched in 2017, Novo Nordisk’s total operating profits are up 60%. Semaglutide product sales grew over 40% last year, accounting for essentially all the corporate revenue expansion. Pharmaceutical demand doesn’t seem to be waning, with Ozempic prescriptions filled globally nearly doubling year-over-year.
2021 FDA approval of the Wegovy semaglutide formulation specifically for weight loss made it the first such drug released since 2104. This could be a huge profit center for Novo Nordisk, who’s targeting 2X sales in this specific treatment category, with a $3.5 billion goal by 2025. Wegovy is now approved for adolescents ages 12 and over, further expanding the potential client pool.
Novo Nordisk is also currently working on a semaglutide pill for obesity, as opposed to the injection format. Meanwhile, Eli Lilly, the second player to enter this market, has countered with Mounjaro and Zepbound, for diabetes and weight loss respectively, both using their proprietary tirzepatide formulation.
Considering the massive market potential, there’s currently an ongoing arms race amongst big pharma battling to get more drugs on the market. Amgen, ERX, Pfizer, and Otsuka are all in early stage of clinical trials for products related to GLP-1-RA.
There has also been an explosion of biotech acquisitions at very rich prices. Any start-up entity with research efforts even remotely tangential to GLP-1-RA technology has seen their valuation skyrocket, as larger players in the pharmaceutical space, who were not previously on the semaglutide train, are now trying to hop on board and quickly catch the leaders. At this rapid rate of development, considering the potential profits at stake, scientific corners will inevitably be cut, despite the best efforts of global regulatory bodies.
Ironically, in public messaging, Novo reps make sure to note they don’t recommend Ozempic be used by anyone other than diabetics. Type 2 diabetes is adult onset, and based on lifestyle decisions, so diagnosis can be somewhat subjective.
While estimates vary widely, at the end of 2022, it’s thought that over 9 million individuals had prescriptions for GLP-1-RA medicines, with the breakdown of diabetes versus weight loss motivation being more difficult to discern. As this tally has tripled in a 3-year span, there’s no doubt even more folks are taking this family of drugs now than when the count was last conducted.
Still, there’s a substantial runway for further product growth. If the cost and availability improve, with 96 million American’s classified as prediabetic by the CDC, over 1/3rd off the adult population, then there’s a huge potential for further pharmaceutical profits.
GLP-1-RA patients have demonstrated reduced calorie consumption by 20 – 30%. This change is substantially skewed to snacks and booze intake, which drop by half or more, according to research by Morgan Stanley. [REF]

This report, which is clearly bullish on the benefits of this new drug category, predicts that by 2035, 24 million people, or 7% of the U.S. population, will be using GLP-1-RA treatments for weight loss. This projected change in consumption habits amongst a broad swatch of consumers could drastically influence some major U.S. consumer packaged goods firms.
For every action, there is an equal and opposite reaction. If Americans are eating and drinking less, who are the losers? Clearly, any company selling sinful swill. Which happens to be some of the largest corporations in the country.
Will revenue for snack food conglomerates be influenced, or can they adjust their business model? Will customers pay more for alcohol, if they are consuming less of it? Will fast food chains be able to engineer their menu items to offset the effects of mental hunger suppression?
Companies like Coca Cola, General Mills, McDonalds, Kraft-Heinz, PepsiCo, Dominos, and Hershey’s have been cornerstones of the U.S. food and beverage landscape for decades. It’s unlikely that these operations will simply disappear, considering how many demographic changes they’ve weathered in the past. In fact, some elements of the quintessential American experience are based on consuming their products, in the kitchen, car, or corner store.
Worrisome Wildcards:
Obviously, there’s no miracle cure, especially for something as complex as obesity. But semaglutides and similar chemistries look pretty close to perfect on the weight loss front, based on all the studies which have been completed to date.
It’s important to look at the detrimental side effects of these drugs, both already known, as well as hidden issues, which could materialize in the future. Ironically, the magic of the GLP-1-RA system, with multiple modes of manipulating the human body, may be their greatest drawback as well.
Of course, first to address are the physical problems associated with modifying the stomach’s normal digestive functioning. Gastrointestinal challenges and bouts of nausea are the most common complaints from semaglutide treatments observed to date. However, these inconveniences don’t seem major; the main reasons that trial patients stopped using the medicine are access and cost. More on that problem to come.
One specific side effect which has materialized recently, albeit infrequently, is gastroparesis. Translated literally from the Greek roots, this literally means stomach turning to stone. While occurring in a low percentage of patients, major digestive issues like pancreatitis, bowel obstruction, and the aforementioned gastroparesis, are shown to be more prevalent in GLP-1-RA patients than the bupropion-naltrexone control medication, at a statistically significant level. [REF]

Another complain from some medical practitioners is that GLP-1-RA treatments are just a glorified fasting tool. Most individuals who go off the medication end up gaining all the weight back fairly quickly, returning to their original meaty physique within a year after stopping injections. This result suggests that these new drugs are not addressing the root cause of the obesity problem. Apparently, the appetite satiation is temporary, not permanent.
Of course, pharmaceutical companies are happy to pedal products that result in captive customers for the remainder of their lived longevity.
Another complaint is with the amusingly dubbed “Ozempic face”. This condition, characterized by flabby skin on a gaunt bone structure, turns out to simply be a product of swift weight loss, and not specifically related to semaglutide intake. These treatments are just the first time that a large quantity of citizens have been able to experience such a rapid reduction in fat content over a very short time period. This effect will clearly require additional messaging.
Other skeptical doctors sight concerns about the fundamentals of human aging. It’s well understood in the medical community that increasing muscle mass is critical for health in old age, in an effort to avoid the effects of sarcopenia. The trade-off of more muscle development is higher insulin levels, which can increase cancer risk.
Studies show that GLP-1-RA treatments cause fat and muscle loss evenly; this is essentially the same phenomenon as starvation. An ideal weight loss miracle cure would be to eliminate the visceral fat around internal organs, which can lead to all manner of chronic diseases, without affecting any other muscle, tissue, or bone properties.
In reality, GLP-1-RA based systems are very young from a drug development standpoint. Researchers are still grappling to understand the side effects, if any; this thorough exploration will take a substantial amount of time to play out. Even if there are long-term downsides, these may be outweighed by reduction in death from obesity-linked causes.
Physical ailments are just one factor. For semaglutides, there’s a brain function shift, which may be even harder to quantify.
Fundamentally, GLP-1-RAs turn off the reward center of the brain. It’s obvious how flipping this switch could lead to issues with sadness, depression, and maybe even suicide. This phenomenon has been observed in other mind manipulation medications of the past.
Then, there’s the unknowns related to messing with the body’s important dopamine signals. Positive versus negative feedback. A brief burst of euphoria versus a pleasant continuous trickle. Short term compulsions versus long term habits. These changes could be beneficial or bad, depending on the mental mechanism being modified. Lots of clinical research will be needed to come up with a conclusive finding on this front.
Well in the future, and even more dystopian, is the potential to influence human will power through GLP-1-RA injections. Is it possible to use this technology to motivate people throughout their daily lives, or even force them to execute acts they typically wouldn’t? The line between reality and science fiction is blurring rapidly.
Where To, Which Way:
There have been other silly health crazes in the past, like master cleansing, electronic muscle stimulation, cold plunges, and oxygen bars. And other diet fads, like paleo, plant-based meat, intermittent fasting, and supplement shakes.
The medical field of semaglutides, trizepatides, and other yet-to-be-discovered chemistries, offers up many of the same compelling traits as these prior phenomena. With momentum, shortages, and cost conspiring to make this modern weight loss method alluring to a broad and gullible swath of society. It will be interesting to see how this burgeoning industry plays out.
No one can debate the potential for substantial health insurance savings, if America as a whole becomes healthier. The real question is how to execute, and fund, this desired result.
While these new weight loss drugs are extremely expensive, price will inevitably come down as generics become available. What’s needed is a thorough cost-benefit analysis. How does a preemptive, proactive, preventative solution to obesity stack up against a passive, procedural, post-issue strategy?
It’s important to have a candid discussion about who is profiting from these treatments, and who is covering the cost. At some point, leaders in either the public or private sectors, with potentially collaboration, will need to make these tough decisions.
Semaglutide treatments for weight loss are not currently covered by Medicare, but all Federal employees are eligible. It will be interesting to watch how legislative policy changes materialize in this realm moving forward.
Could the government help fund this health transformation, through intervention or subsidies? Sure. Except the national budget is currently way underwater already, and not headed closer to the green side of the ledger any time soon.
Granted, there’s currently lots of money already being spent by the administration on much less beneficial programs. Healthcare is a polarizing political issue, which requires considering second-order effects, and long-term consequences; both factors which live-in-the-present government officials are not great at grasping.
One of the main future challenges with these GLP-1-RA weight loss drugs is equity of access. There are already concerns about creating issues with nationwide healthcare discrimination, as rich people are generally afforded broader and better medical resources. High-cost wellness treatments accessible just to the affluent will only widen this divide. Unfortunately, the poor segment of society is where obesity issues are most acute.
Some doctors propose that fixing the food supply, by reducing daily sugar intake, could be a more efficient and cost-effective solution. However, this approach is difficult from a government leadership standpoint. The last major nutrition mandate by United States scientific leadership suggested a crazy pyramid of high starch and low protein intake. Which is exactly how we got into this obese, diabetic, mess. [REF]

Confidence isn’t high in the U.S. administrative ranks to make the right decisions, especially in this modern era of polarization. Scientific progress has guided civilization through many difficult challenges in the past. Thus, we may need to lean heavily on the private sector. And simply hope righteous humanitarian ideals outweigh ruthless capitalistic greed. It never hurts to be optimistic. A term which is undoubtably part of Ozempic’s unique naming construct.
Especially during the fun and festive holiday season, then the rigid resolutions associated with turning over of the calendar, new and novel weight loss drugs will continue to garner the spotlight. If a family member is looking a little thinner than usual, and eating a lot less, then they may be early to the semaglutide party.
Missing out on roast beef, cheesy potatoes, fig pudding, and red wine, doesn’t sound very fun. At least there will be plenty of topics to keep spirited dinner table conversation going.
Whole Truth:
-
Background on the complex process for pharmaceutical drug naming. [REF]
-
The sophisticated science of semaglutides. [REF]
-
Detailed global obesity statistics, broken down by country. [REF]
-
Lots of body metric data for Americans from the CDC. [REF]
-
List of absurd modern health trends. [REF]
-
Stats on the amazing growth of GLP-1-RA injections in the United States. [REF]
-
2-part Plain English podcast by Derek Thompson which provides a thorough summary of GLP-1-RA technology in audio form. [REF]